胃内脱気水充満法と超音波内視鏡検査
超音波内視鏡の胃内脱気水充満法の起源
超音波内視鏡の胃内脱気水充満法の歴史
経食道断層心エコー法(1977、ref.1)及び超音波内視鏡検査法(1978、ref.2)はいずれも久永等により世界に先駆けて開発されたものです(ref.1~ref.3)。 経食道2Dスキャンナー装置と超音波内視鏡スキャナー装置はいずれもメーカーの援助は全く受けておらず、久永が単独で開発し、安全性は久永及びその共著者がフレキシブルチューブ付きのプローブを多数回自ら飲み込み、確かめたものです。
多数の正常者及び患者での検査の結果、超音波内視鏡検査においては時として診断能ある高解像度の断層像が得られないことが判明しました。 これは久永等が開発したようにトランスデューサ―の回りに液体を充満したバルーン(あるいはオイルバッグ)を設置することである程度は改善されますが(ref.3A, ref.5, ref.6, ref.9, ref.10)、確実に安定した断層像を得るには胃内脱気水充満法が必要であることに気付きました。
この脱気水充満法は久永等により世界で初めて1980年に報告されたものであり(ref.12, ref.13)、これなくして多層の胃粘膜を観察することはできまん。 超音波内視鏡を世界で初めて開発し、検査したといっている研究者は日本及び外国に多数いますが、Hisanaga以前に開発し検査を行ったのは誰もいません。
驚いたことに胃内脱気水充満法に関しては、1980年日本超音波医学会における久永の胃内脱気水充満法(ref.12)の発表時、北の方の大学の教授が座長に促されて檀上に上り、「胃カメラ検査で水の服用を禁じるのは常識で、極めて危険だ」と久永を非難しました。非難したにもかかわらず、この4~5年後、この教授が胃内脱気水充満法は自分が最初に行ったかの如く英文雑誌で発表したのには本当に驚きました。日本の学者も外国の学者と同様にびっくりするような恥ずかしい発表をなさいます。 ところで、胃内脱気水充満法などという変な言葉は久永以外に作る人はいないでしょう。
時間に余裕のある方はこちらもご覧ください。
History of endoscopic ultrasonography. ここをクリック
History of transesophageal echocardiography. ここをクリック
History of echocardiography. ここをクリック
References
1. Hisanaga K, Hisanaga A, Nagata K, Yoshida S A new transesophageal two-dimensional echocardiographic system using a flexible tube and its clinical applications. Proceedings of Japan Society of Ultraonic in Medicine 32:43-44, 1977

From Ref.1 Transesophageal horizontal scan in a normal adult.
2. Hisanaga K, Hisanaga A. A new trans-digestive-tract scanner with a gastrofiberscope. Proceedings of the 23rd Annual Meeting of American Institute of Ultrasound in Medicine. p.108, November, San Diego, 1978
3. Hisanaga K, Hisanaga A. A new real-time sector scanning system of ultra-wide angle and real-time recording of entire adult cardiac images --Transesophagus and Trans-chest-wall methods --. In:White DN, Lyons AE, eds. Ultrasound in Medicine. Vol.4. New York; Plenum Press, pp391-402, 1978

From Ref.3 Insertions of transducer to esophagus and transesophageal ultrasound examinations were performed with patients in left lateral position(left). Typical horizontal scan in a normal adult by using transesophageal method(right).

From Ref.3 Transthoracic image. A long axis scan in a 31-year-old normal man. Entire heart image is seen. The endocardium of the left ventricle and the right ventricular anterior wall are seen.

From Ref.3 Transesophageal M-mode echograms. These images were recorded in order to identify echo sources of transesophageal cross-sectional images shown in Fig.10. Arrows A,B and C of Fig.10A and Fig.10D correspond to Fig.9A, 9B and 9C in each and show directions of M-mode echograms.
3A. Hisanaga K, Hisanaga A transesophageal real-time sector scanner with an oil filled cell. Proceedings of the 23rd Annual Meeting of American Institute of Ultrasound in Medicine. p.47, November, San Diego, 1978
4. Hisanaga K, Hisanaga A, Nagata K, Ichie Y. A trans- stomach wall sector scanner with a gastrofiberscope.
Abstract of 2nd WFUMB, p383, July 22-27, Miyazaki, 1979
5. Hisanaga K, Hisanaga A, Nagata K, Ichie Y. A trans- stomach wall high speed rotating scanner and initial clinical results. Proceedings of the Japan Society of Ultrasoics in Medicine 35:115-116,1979

Photography of original paper.

From Ref.5 Trans-stomach-wall high speed rotating scanner.

From Ref.5 Horizontal scan through the left kidney in a normal adult by using the trans-stomach-wall rotating scanner. When
near gain is standard, pancreas is seen as echo free space near the stomach.
6. Hisanaga K, Hisanaga A. High speed rotating scanners for trasesophageal echocardiography and transgastoric sonography. Eizou Jouhou Medical 11:1094-1099, 1979 (In Japanese)

From Ref.6 Transgastric high speed rotating scanner with flexible tube.

From Ref.6 Horizontal scan at the level of kidney in a normal adult. Pancreas is seen very clearly.
7. Hisanaga K, Hisanaga A. Pancreatic echography using a trans-stomach wall ultrasound rotating scanner (abstr). Gastroenterology 78:1183, 1980
8. Hisanaga K, Hisanaga A, Kambe T. An endoscopic ultrasound scanner for abdominal echography (abstr). Gastrointestinal Endoscopy 26:68, 1980
9. Hisanaga K, Hisanaga A, Nagata K, Ichie Y. High speed rotating scanner for transgastoric sonography. Am.J.Roentgenol. 135:625-629, 1980
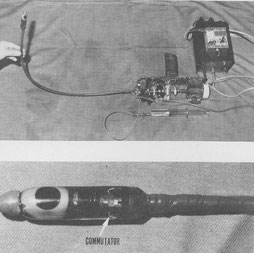
From Ref.9 Upper Fig. Intragastric high speed rotating scanner. Small transducer in stomach is rotated by flexible rotating shaft and motor at 15-50 cycles/sec.Lower Fig. Transducer and commutator in oil bag.


From Ref.9 Horizontal scans through left kidney in normal adult with intragastric high speed rotating scanner. Left : Left kidney and abdominal aorta are seen clearly. If amplitude of near field is relatively low, pancreas is seen as anechoic space near stomach wall. Right : With increasing amplitude of near field, pancreas assumes cloudlike shape.
10. Hisanaga K, Hisanaga A, IchieY, Hibi N, Nishimura K, Kambe T. High speed rotating scanner for transesophageal cross-sectional echocardiography. Am. J. Cadiol. 46:837-842,1980

From Ref.10 Diagrammatic illustration of the transesophageal high speed rotating scanner. A small transducerin the esophagus is rotated througha a full 360° through a flexible shaft by a motor at 15 to 50 cycles /s. Although the small transducer is rotated with great speed in the patient's esophagus, no damage results because the transducer is safely enveloped in an oil bag.

From Ref.10 Transesophageal high speed rotating scanner.

From Ref.10 Transducer and commutator in oil bag. Sound energy is coupled to and from the transducer through the slip-ringcommutator because of the full 360° rotation of the transducer.


From Ref.10 Transesophageal cross-sectional echocardiograms in a patient with mitral stenosis. The cross section is horizontal and shows the heart as viered from the cardiac apex. A : a frame during diastole and B : a frame during systole. Interatrial septum (IAS) is seen without dropout. AML= anterior mitral leaflet, ESO = esophagus, IVS = interventricular septum, LA = left atrium, LV = left ventricle, PML = posterior mitral leaflet, RA = right atrium, RV = right ventricle, TV = tricuspid valve.
11. Hisanaga K, Hisanaga A, Nagata K, IchieY. Transesophageal cross-sectional echocardiography. Am. Heart J. 100:605-609,1980

From Ref.11 Transesphageal horizontal scan at the level of the aortic valve . The aortic cusps are closed in diastole. Large left atrium is seen. Right ventricular outflow tract is seen anterior to the aorta. AV = aortic valve, RVOT = right ventricular outflow tract.

From Ref.11 Transesophageal vertical linear scan through the pulmonary artery in a normal subject. Bifurcation of pulmonary artery and part of ascending aorta are seen. AO = aorta, PA = pulmonary artery , BI = bifurcation of pulmonary artery.
12. 久永光造、久永朝香、神戸忠 内視鏡的超音波断層法の検査手技と腹部断層像の同定(その2)-胃内脱気水充満法についてー 日本超音波医学会講演論文集 37:413-414, 1980

Photography of original paper.

From Ref.12 Horizontal scan through the stomach posterior wall in a normal adult by using the transgastric sector scanner with gastrofiberscope when the stomach was filled with water. Left kidney is seen clearly. SW = stomach wall, LK = left kidney, V = vertebra, R = right, L = left.
Content of this paper is filling stomach with water during EUS examination in order to increase acoustic contact between stomach wall and transducer. Hisanaga performed this method for the first time in the world certainly. This is the most important discovery in EUS examination.
13. 久永光造、久永朝香 超音波内視鏡の検査手技 ー消化管内脱気水充満法についてー、 映像情報メディカル 12:773-776、1980